The Economy of Slave Reproduction
“Ophelia Whitley remembered that in rare instances, her master would force parturient women to “go ter de house an’ find a baby an’ be back at wuck de next day.” [1]


It is important to understand the basis for medical interest in Black women specifically, which only increased throughout the 18th and 19th centuries. Virginia banned the transatlantic slave trade in 1778 alongside other states” [2] Thus, the legal acquisition of foreign slave labor ceased to be a viable option. Enslavers instead turned their attention to Black women already in the Americas; they had a vested interest in the reproductive health of their female slaves as it became integral to the slave economy.[3] The tragic result of this was forced coupling at young ages with some women bearing as many as twenty children in their lifetime.[4] These women were consequently subjected to both the care and curiosities of medical professionals meant to safeguard that reproductivity. Even British practitioners like Dr. Collins lent their “expertise,” advising readers on how to maintain “healthy and productive” enslaved African laborers.[5] Enslaved women’s exposure to medical practitioners, coupled with their vulnerable social position, made them popular victims for experimentation.
Harvard College, the College of William and Mary, and Yale were the first three universities of substance to be established in the British North American colonies.[6] These centers of learning proceeded to reinforce the slave-driven economy that it existed within as slaveholders committed their money and children to these institutions.[7] For as the colonies matured, its merchant class of slaveholders became more intimately intertwined with higher education. In the antebellum era, for example, cotton planners largely funded the expansion of universities for both the North and South.[8] The unsurprising result of this was an increasing intolerance for anti-slavery sentiments. As the son of slave owners and a student of medicine, Richard C. Mason was no doubt shaped by these factors.
It is important to note that some historians assert universities in the antebellum South were neither organized nor racially motivated in their targeting of Black individuals. Instead, enslaved Blacks were subject to experimentation because of their availability.[9] Furthermore, some have posited that medical schools sought out legitimately ill slaves within the legal system.[10] They then delivered experimental treatment with the purpose of successfully healing them.[11] In this interpretation, slaves are reframed not as blatant test subjects but ill people already in need. The slaves are dictated some autonomy with claims that the slave patients were eager to be treated.[12] As stated above, however, the availability of Black test subjects for experimentation and observation was largely race-based.
The crushing and unrealistic demands of slaveholders often necessitated medical treatment in the first place. Their desire to maximize their profits with self-reproducing slaves subjected enslaved women to terrible circumstances where they were forced to work after delivering yet another child. This in itself places them directly at risk for an array of health complications. The institutions funded by enslavers would reinforce the attitudes of these patrons nonetheless. Thus, Blacks remained particularly vulnerable to abuse or mishandling at the hands of researchers, medical teachers, or students.[13]
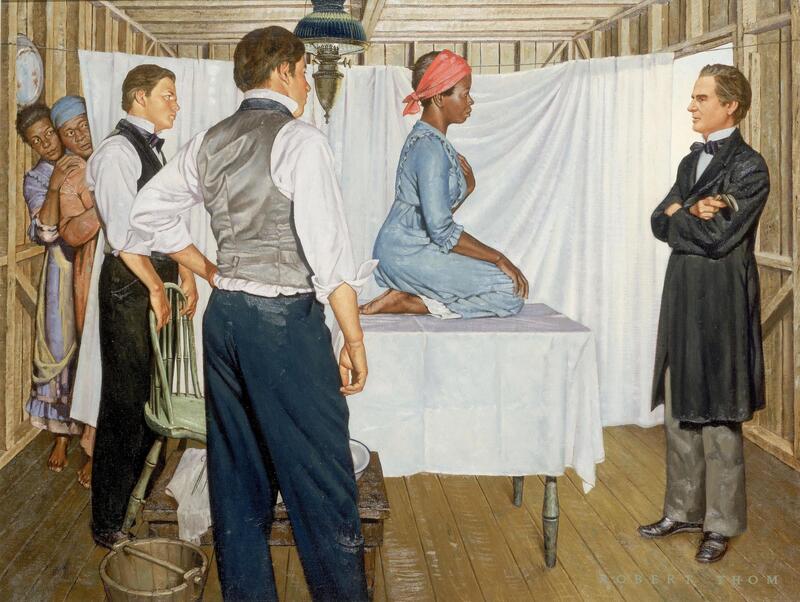
Dr. Sims is regularly regarded as the Father of Gynecology.[14] He spearheaded medical breakthroughs using enslaved Black women as part of his research, performing as many as thirty experimental surgeries on them.[15] Worse still, the man trained his patients to act as nurses and assist him as he performed additional surgeries on their compatriots.[16] When Dr. Sims died, his eulogy embraced the narrative that these women were happy to serve the advancement of gynecological research.[17] One must address this stance with a critical eye. The assumption that enslaved Black women would willingly subject themselves to experimentation is just as easily interpreted as a fabrication meant to soothe the conscience.[18]
It should also understand that Dr. Sims repeatedly claimed Black women recovered from the same operations faster than their white counterparts.[19] He was not alone in this assertion, which so conveniently fed into the desire of many enslavers hoping to return their recently pregnant female slaves to work. This impulse to distinguish Black women as particularly hardy is therefore another consequence of racist ideology. A modern audience can best understand this concept as the construction of “medical superbodies." [20]
Medical superbodies allowed medical professionals and enslavers to disregard the agony enslaved Black women endured as tolerable, even noble. Antebellum medicine could then reinforce this notion by defining the “normal” and “finer” nervous systems of, which were grafted onto elite white women.[21] Any deviation from this normality was to be an indication of racial inferiority from Black, poor, and immigrant women alike.[22] It is this attitude that inevitably informed Richard C. Mason’s dissertation and subsequent assumptions about female anatomy.
The misguided and blatantly false assumptions of medical professionals continued to have a very real impact on the lives of black individuals. The case of the Almshouse v. Alexander Whistelo in 1808 illustrates this exactly. Experts of various medical backgrounds were called into court to settle the matter of paternity, for a woman of mixed heritage produced a fair child after being assaulted by both a Black and white man. The judges took sworn testimonies from these medical professionals, and it is their collective understanding of biology that ruled the Black assailant could not have fathered the child. Andrew Duncan was one such witness, and his continued involvement in court cases both criminal and civil serves as yet another testament to the influence doctors wielded. It is unsurprising, then, that Richard C. Mason was himself called to testify in court when a local slave patrol.
[1] Deidre Owens, In Medical Bondage: Race, Gender, and the Origins of American Gynecology (Athens: University of Georgia Press, 2017), 118.
[2] Dea Boster, "An "Epeleptick" Bondswoman: Fits, Slavery, and Power in the Antebellum South,” Bulletin of the History of Medicine 83 no. 2 (2009), 19.
[3] Boster, “An Epeleptick,” 19.
[4] Owens, In Medical Bondage, 109.
[5] Rana A. Hogarth, Medicalizing Blackness: Making Racial Difference in the Atlantic World (CHAPEL HILL: University of North Carolina Press, 2017), xi.
[6] Steven Wilder, Ebony and Ivy : Race, Slavery, and the Troubled History of America’s Universities, (New York: Bloomsbury Press, 2013), 17.
[7] Wilder, Ebony and Ivy, 18.
[8] Wilder, Ebony and Ivy, 182.
[9] Savitt, “The Use of Blacks,” 331.
[10] Savitt, “The Use of Blacks,” 342.
[11] Savitt, “The Use of Blacks,” 342.
[12] Savitt, “The Use of Blacks,” 344-345.
[13] Savitt, “The Use of Blacks,” 348.
[14] Deidre Owens, In Medical Bondage: Race, Gender, and the Origins of American Gynecology (Athens: University of Georgia Press, 2017), 108.
[15] Savitt, “The Use of Blacks,” 344.
[16] Owens, In Medical Bondage, 114.
[17] Owens, In Medical Bondage, 109.
[18] Owens, In Medical Bondage, 108.
[19] Owens, In Medical Bondage, 109.
[20] Owens, In Medical Bondage, 109.
[21] Owens, In Medical Bondage, 115.
[22] Owens, In Medical Bondage, 115.